

Background: Lenalidomide (LEN) monotherapy has been effective in extending progression free survival (PFS) after AuSCT in pts with MM. Elotuzumab (ELO), a humanized IgG1 immunostimulatory monoclonal antibody against signaling lymphocytic activation molecule F7 (SLAM F7), is FDA approved in combination with LEN and dexamethasone (DEX) for treatment of MM pts who have received 1-3 prior therapies. We report updated results of this phase 2 trial evaluating the efficacy and safety of adding ELO to LEN as maintenance therapy post- AuSCT.
Patients and Methods: Between 4/15/2015-1/27/2016, 27 evaluable pts were treated on 28 day cycles with ELO, 10 mg/kg iv weekly for cycles 1-2, q2weeks for cycles 3-6, then 20 mg/kg once monthly for cycles 7+. Pts enrolled after 1/28/2016 (n=73 pts) have received ELO, 10 mg/kg IV weekly for cycles 1-2, and 20 mg/kg on day 1 from cycle 3 until disease progression (PD). LEN has been dosed at 10 mg/day for cycles 1-3, with a dose increase to 15 mg/day at physician discretion starting with cycle 4, in the absence of non-hematologic toxicity > grade 1 and significant cytopenias (ANC < 1000/mL, platelet count < 100,000/ml). For the 1st 8 weeks, pts <75 yrs receive 28 mg of DEX 3-24 hours pre-infusion, while pts ≥75yrs receive 8 mg; pts receive 4-10 mg iv DEX pre-infusion for all cycles. Zoster and thromboembolic prophylaxis is prescribed, commensurate with standard recommendations.
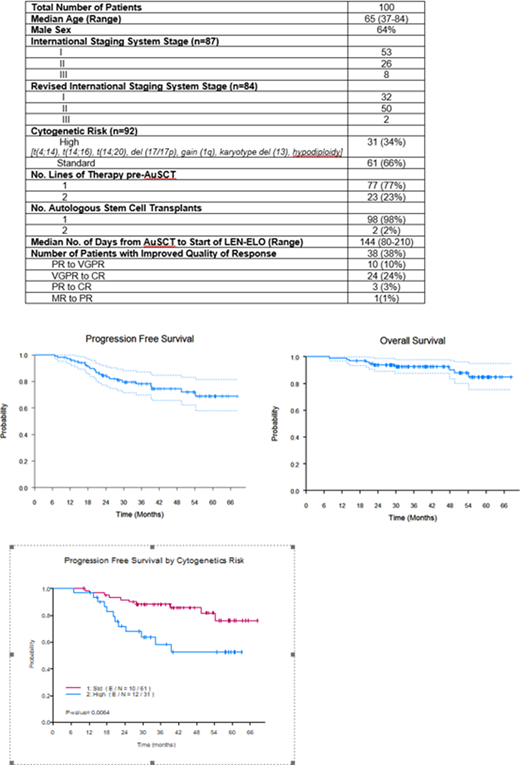
The study's primary endpoint is PFS, defined as time from AuSCT to PD or death (whichever occurs first), or censored at date of last contact. Secondary objectives are best response, OS, incidence of second primary malignancies (SPMs) and adverse event (AE) profile. Total enrollment of 100 evaluable pts was completed on 6/5/2019. Patients are followed until death, withdrawal of consent or removal from study. Eligible pts received ≤2 lines of induction therapy, and were 60-210 days post-AuSCT.
Results: Pts (n=100) have been treated for a median of 27.5 cycles (4-67). At study entry, 37 (37%) had complete response (CR), 40 (40%) very good partial response (VGPR), 22 (22%) partial response (PR) and 1 (1%) minor response (MR). Best response achieved to date on study is CR in 61 pts (61%), VGPR in 29 pts (29%) and PR in 10 pts (10%). Median time for conversion to CR on study is 1 month. Of pts in CR and tested for minimal residual disease (MRD) to date, 42/48 are negative (flow cytometry on ≥ 2 x106 cells). Eleven of 42 have converted from VGPR to MRD negative CR while on study.
With a median follow up of 41 months, 90% of pts (n=90) remain alive. Eighteen pts have had PD; of these, 10 had high-risk cytogenetics. Three died of PD while receiving salvage therapy, 1 of pneumonia, 4 of second malignancies and 1 of unknown cause at another facility. One additional pt died on study in VGPR, after developing acute cerebral encephalopathy with refractory status epilepticus of unclear etiology. Estimated 4 year PFS is 75%. High-risk cytogenetics (n =31) adversely affected PFS (p=0.01); 14/31 pts remain on study. Of 23 pts transitioned to another therapy, median 2nd PFS has not been reached.
Grade 3-4 Hematologic AEs (no. of pts/102 pts) were: neutropenia 32% (33), febrile neutropenia 15% (15), thrombocytopenia 7% (7), and anemia 10% (10). Grade 3-4 non-Hematologic AEs (no. of pts): hypophosphatemia 29% (30), respiratory infections 21% (21), diarrhea 15% (15), fatigue 12% (12), peripheral neuropathy 8% (8), other infections 7% (7), myalgias 5% (5), dyspnea 5% (5). SPMs include cutaneous basal and squamous cell carcinomas (8), AML (1), B-cell ALL (1), t-MDS (4), osteosarcoma (1), intra-epidermal adenocarcinoma of the neck (1), mucinous appendiceal neoplasm (1), mucinous epidermoid carcinoma of parotid (1), prostate cancer (1). Renal cell carcinoma was diagnosed in 1 pt, 15 months after removal from study for PD.
Conclusions: Lenalidomide-elotuzumab is a well-tolerated maintenance therapy on which 38% of pts have had improvement in quality of response while on therapy, including 27% who converted to CR. SPM rates seem consistent with those observed in CALGB 100104 and IFM 2005-02 trials of lenalidomide alone. Longer follow up is required to determine how median PFS and OS will compare with those from lenalidomide monotherapy trials, and how SPM rates will continue to evolve.
Thomas:X4 Pharma: Research Funding; Ascentage: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Xencor: Research Funding; Pharmacyclics: Other: Advisory Boards; Genentech: Research Funding. Shah:Karyopharm: Current Employment, Current equity holder in publicly-traded company. Lee:Regeneron: Research Funding; Daiichi Sankyo: Research Funding; Sanofi: Consultancy; GlaxoSmithKline: Consultancy, Research Funding; Genentech: Consultancy; Takeda: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Genentech: Consultancy. Manasanch:JW Pharma: Research Funding; Merck: Research Funding; Quest Diagnostics: Research Funding; Takeda: Honoraria; BMS: Honoraria; Glaxo Smith Kline: Honoraria; Adaptive Biotechnologies: Honoraria; Novartis: Research Funding; Sanofi: Honoraria, Research Funding. Patel:Oncopeptides: Consultancy; Takeda: Consultancy, Research Funding; Cellectis: Research Funding; Bristol Myers Squibb: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Nektar: Consultancy, Research Funding; Precision Biosciences: Research Funding; Poseida: Research Funding. Kaufman:Bristol Myers Squibb: Research Funding; Karyopharm: Honoraria; Janssen: Research Funding. Iyer:Trillium: Research Funding; Daiichi Sankyo: Consultancy; Legend Biotech: Consultancy; Merck: Research Funding; Rhizen: Research Funding; Seattle Genetics, Inc.: Research Funding; Target Oncology: Honoraria; Afffimed: Research Funding; CRISPR: Research Funding; Spectrum: Research Funding; Curio Biosciences: Honoraria. Qazilbash:Angiocrine: Research Funding; Bioclinica: Consultancy; Janssen: Research Funding; Bioline: Research Funding; Amgen: Research Funding. Bashir:Amgen: Other: Advisory Board; Purdue: Other: Advisory Board; Takeda: Other: Advisory Board, Research Funding; Acrotech: Research Funding; StemLine: Research Funding; Celgene: Research Funding; KITE: Other: Advisory Board. Orlowski:Laboratory research funding from BioTheryX, and clinical research funding from CARsgen Therapeutics, Celgene, Exelixis, Janssen Biotech, Sanofi-Aventis, Takeda Pharmaceuticals North America, Inc.: Research Funding; Amgen, Inc., AstraZeneca, BMS, Celgene, EcoR1 Capital LLC, Forma Therapeutics, Genzyme, GSK Biologicals, Ionis Pharmaceuticals, Inc., Janssen Biotech, Juno Therapeutics, Kite Pharma, Legend Biotech USA, Molecular Partners, Regeneron Pharmaceuticals, Inc.,: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi-Aventis, Servier, Takeda Pharmaceuticals North America, Inc.: Honoraria, Membership on an entity's Board of Directors or advisory committees; Founder of Asylia Therapeutics, Inc., with associated patents and an equity interest, though this technology does not bear on the current submission.: Current equity holder in private company, Patents & Royalties; STATinMED Research: Consultancy.
Elotuzumab (ELO), a humanized IgG1 immunostimulatory monoclonal antibody against SLAM F7. It is FDA approved in combination with Lenalidomide and dexamethasone (DEX) for treatment of MM pts who have received 1-3 prior therapies. This is a phase 2 trial evaluating the efficacy and safety of adding ELO to LEN as maintenance therapy post-autologous stem cell transplant.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal